Colorectal Quiz: May 22, 2023
Quiz for May 15th:
What is this cell, and what features determine that conclusion?
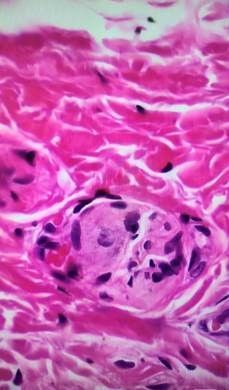
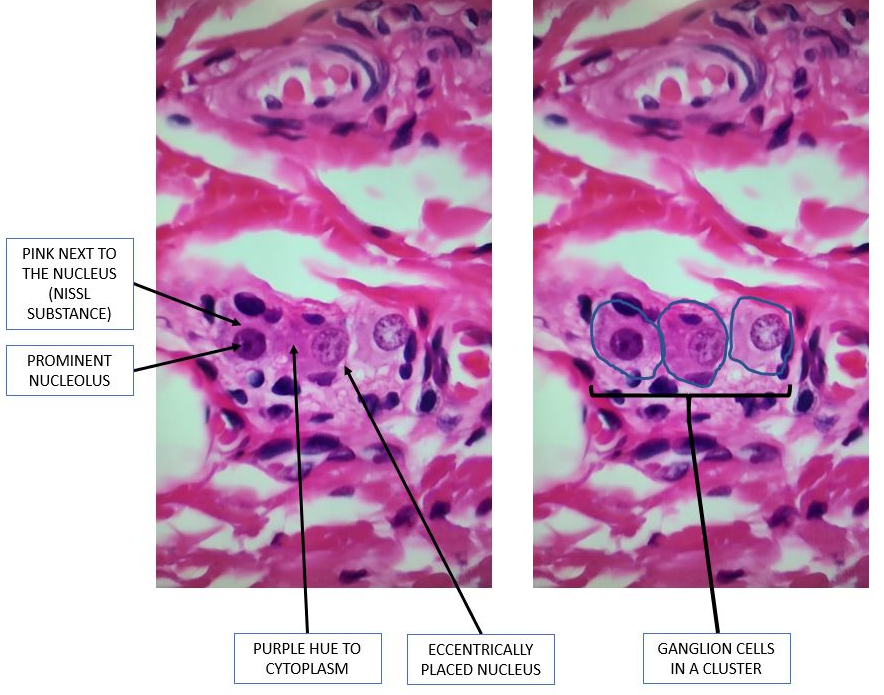
Answer for May 15th Quiz: There are some key features the pathologist looks for in determining what is a ganglion cell. I hope this diagram I have annotated is helpful to you. They tend to form clusters, there is pink next to the nucleus which represents Nissl substance, the nucleolus is prominent, the nucleus is eccentrically located, and there is a purple hue to the cytoplastm.
Quiz for May 22:
A patient comes to you with HD diagnosed at another hospital, with a rectal biopsy, sigmoid biopsy and appendix; all showing no ganglion cells. Based on these biopsies, the hospital determined the patient had total colonic HD. The child is 8-months-old and is doing well on irrigations. How would you proceed?

How would you handle this case?

