Colorectal Quiz: May 15, 2023
Quiz for May 8th:
Here is the distal colostogram of a male ARM who underwent a colostomy at birth. It appears to show a bulbar fistula. But what is curious is the section just distal to the mucous fistula that appears narrow. How would you handle this case? PSARP and deal with the narrow area at the time of the colostomy closure? Resect the distal segment and pull through the proximal colostomy?
Answer for May 8th Quiz: The narrowing distal to the mucous fistula persists on all distal colostogram images. It is hard to know whether this narrowing is significant. I would recommend proceeding with the PSARP for this bulbar fistula. At the time of the colostomy closure would assess this distal segment and possible anastomose the proximal stoma to the upper rectum if this narrowing is real. An alternative approach of removing the distal segment and pulling through the proximal stoma should be avoided given the importance of preserving the rectum.

Quiz for May 15th:
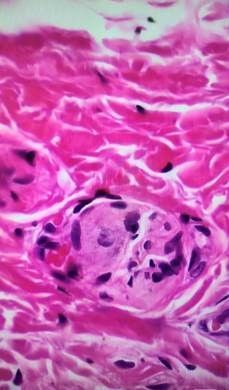
What is this cell, and what features determine that conclusion?
How would you handle this case?

