Colorectal Quiz: July 31, 2023
Quiz for July 24th:
A 6-year-old male presents with severe intractable constipation and failure to thrive. Concern for Hirschsprung disease led to a rectal biopsy which showed no ganglion cells but no hypertrophic nerves. What would you do for this patient?

Answer for July 24th:
This patient seems to have HD clinically, the biopsy needs to be repeated. And his failure to thrive requires a diversion, so I would suggest a repeat rectal biopsy, laparoscopy, biopsy of the sigmoid and ileostomy. He turned out to have HD did very well with the ileostomy, then underwent his pull-through (laparoscopic assisted pull-thru of the ganglionated sigmoid) and thereafter ileostomy closure.
Quiz for August 1st:
3 year old female s/p HD pull-through with perineal abscesses which occurred several months later requiring drainage and seton and diversion with a colostomy. Here is the contrast study of the colostomy, and of the distal segment of the pull-through. What would you do for this patient?
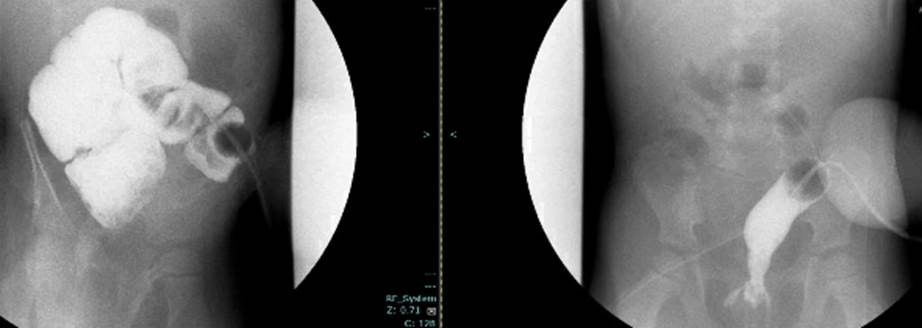
How would you handle this case?

