Colorectal Quiz: August 7, 2023
Quiz for August 1st:
3 year old female s/p HD pull-through with perineal abscesses which occurred several months later requiring drainage and seton and diversion with a colostomy. Here is the contrast study of the colostomy, and of the distal segment of the pull-through. What would you do for this patient?
Answer for August 1st:
Given all that transpired in the pelvis and with the presence of a fistula – this distal segment needs to be removed. Likely a pelvic abscess had developed. Removal of the distal segment requires carving out the lumen, and these are quite stuck to the sacrum. Then the colostomy site can be mobilized for the new pull-through.
Quiz for August 8:
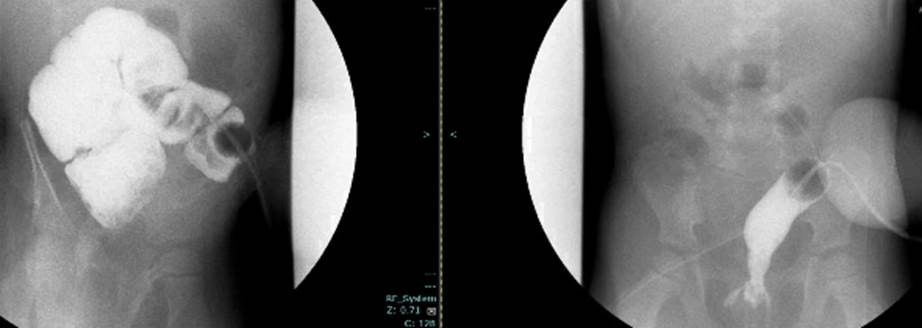
How would you handled the below case, a male with ARM, who underwent a newborn colostomy, and here you see the distal colostogram. What is the malformation and what would be your approach?

How would you handle this case?

