Colorectal Quiz: April 24, 2023
Quiz & Answer for April 17th
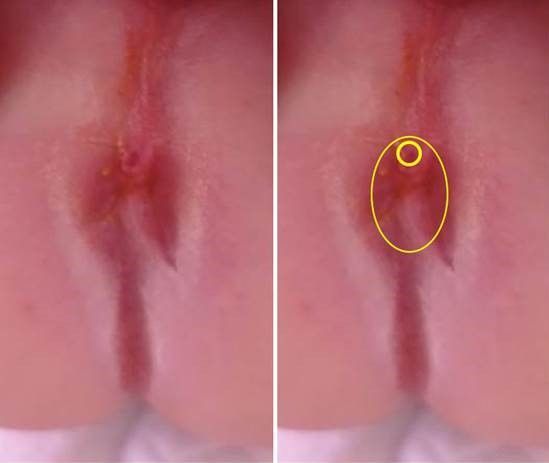
Newborn male with ARM with perineal fistula shown here. We asked what would be your approach for this repair and when would you do this operation?
This case, as it true for almost all males with perineal fistula has the fistula located within the sphincter ellipse, just at it most anterior portion, as you see outlined in yellow. This is a perfect for a posterior only mobilization. There is no need to mobilized the anterior wall of this fistula, and in fact avoiding doing so will eliminate the major complication seen in male rectoperineal fistula repairs – that of a urethral injury. Please see this helpful video:
https://www.expertsinsurgery.com/programs/posterior-rectal-advancement-anoplasty?categoryId=49506
And this article:
Devin R Halleran, David Coyle, Afif N Kulayla, Hira Ahmad, Jacob C Langer, Alessandra C Gasior, Karen A Diefenbach, Richard J Wood, Marc A Levitt. The cutback revisited - The posterior rectal advancement anoplasty for certain anorectal malformations with rectoperineal fistula. J Pedatr Surg. 2022 Sep;57(9):85-88. https://pubmed.ncbi.nlm.nih.gov/35012765/
Quiz for April 24th
The x-ray below is of a 2-year-old male who underwent a redo of their HD pull-through for transition zone. The right colon remained and this was pulled through down the right pelvis. They started stooling well on postoperative day #3 and were started on a diet. On postoperative day #5 they began to have abdominal distension and emesis. Based on these symptoms and this x-ray, what do you think is the problem and what would you do?

How would you handle this case?

