Colorectal Conundrum: October 23, 2023
For the Quiz & Answers to last weeks Conundrum - see the blog post here.
Colorectal Conundrum for October 23rd:
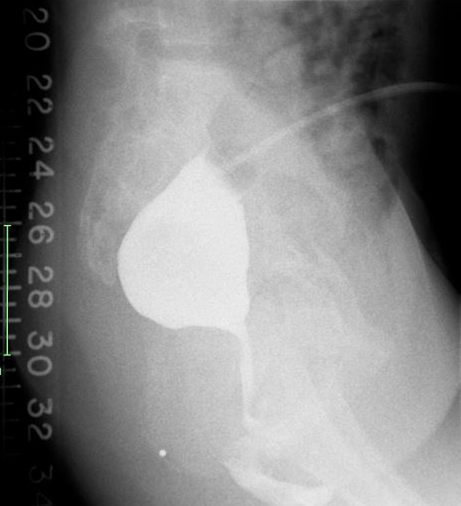
12 year old female with an anorectal malformation, underwent a colostomy as a newborn, and has never been repaired. On exam she has a tiny fistula visible at the vestibule. A distal colostogram is shown. She also has a loop ureterostomy placed for distal ureteral obstruction. What is your diagnosis and what is your operative plan?
Answer for October 23rd:
I hope you were not fooled by this image. Some might wrongly conclude that this is a bulbous high rectum with a long narrow fistula. But in fact this is a non-distended distal rectum and in fact the distal rectum is within mm of the perineal skin. It is not common to see a distal colostogram in a patient with a vestibular fistula and certainly not one that had never been repaired until the age of 12. A posterior sagittal approach can be planned, and utilizing the new perineal body sparing technique. For this approach see this video:
How would you handle this case?

