Colorectal Quiz: September 4, 2023
Quiz for August 28th:
Based on last week’s quiz, a baby girl with ARM and rectovestibular fistula who was taken to the OR for a PSARP and found to have distal vaginal atresia – with laparoscopy performed showing an atretic left Mullerian system with normal ovary, and what appeared to be a unicornuate uterus on the right with potentially a blind ending distal vagina in the pelvis. What would you do now?
A. PSARP only, leave the Mullerian system untouched
B. PSARP plus vaginal replacement using the distal rectum
C. PSARP plus vaginal replacement using sigmoid, keep the distal rectum as rectum
D. Pull-through of native left vagina to perineum
E. Something not listed above, I would do___________________________.
Answer for August 28th:
Via PSARP we were able to find quite easily the blind ending distal vagina. (Answer D). We decided to suture this into the perineum and did not open the lumen, reconstructing the perineal body and performing an anoplasty. In the future, at puberty we anticipate we will do an introitoplasty once this structure dilates up.
Quiz for September 4th:
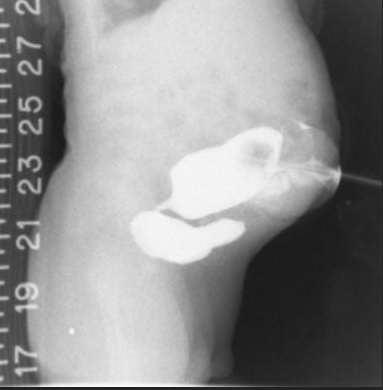
Another interesting distal colostogram in an ARM male patient who had a newborn colostomy. What would you call this malformation and how would you approach the reconstruction?
Answer for September 4th:
This is a rare case of a rectovesicle fistula. A laparoscopic approach is ideal. It is hard to tell from this image whether there is enough distal bowel for the pull-through, but on other images there is enough, so that a laparoscopic mobilization should get the distal rectum to reach.
How would you handle this case?

