COLORECTAL QUIZ: May 9, 2022
Happy Monday.
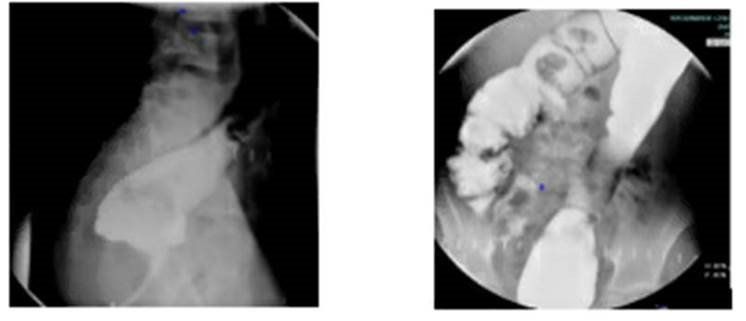
Last week, I asked you about a 16 year old male with HD, previous redo pull-through for a retained cuff at age 11. He stools three times a day, somewhat soft consistency, and often has urgency, and occasionally has a soiling accident. He is not distended and has not had any episodes of enterocolitis since his redo. His contrast enema and plain abdominal xray is below. His exam showed no stricture and an intact dentate line, and no residual cuff. The biopsy at the time of the redo was normal.
What would you recommend for his treatment?

I received this awesome reply from Krystal Artis one of our Pas, and Katie Worst, one of our NPs:
“It appears that there should be no anatomical concerns with providing him bowel management. His abdominal x-ray looks free from stool accumulation and burden. Taking into consideration that he is not currently on any regimen, this suggests that he has some degree of hypermotility and he would most benefit from some "bulking" of his stools. This will hopefully decrease the "urgency" associated with his bowel movements as well as the frequency. We would recommend providing the family with dietary guidelines and asking them to lean more towards constipating foods as well as starting fiber supplementation with a water soluble product such as Citrucel or Metamucil. We also would ask this patient to try pelvic floor physical therapy due to concern that he may not be emptying completely each time he uses the bathroom because he typically has multiple trips. It would be helpful to make sure that he is fully relaxing his sphincters when sitting.”
I agree – this patient has an intact continence mechanism, and an empty colon, and stools 3 times per day, mostly loose. He needs some bulk to his stool. No need for a biopsy, no need of course for a redo, and no need for a Malone, just a better bowel regimen as Krystal and Katie have outlined.
OK, for this week:
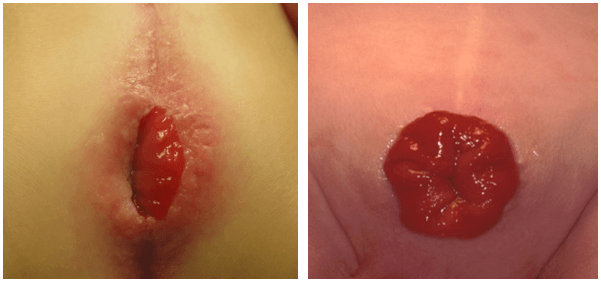
Here are to rectal prolapses after a PSARP, in two different patients. Both under one year of age.
New Paragraph
How would you handle this case?
Here is the current list of the Colorectal Quiz podcasts, best viewed via the StayCurrent app:
Colorectal Quiz Episode 1 ARM - Low Bulbar Fistula, https://staycurrentapp.app.link/wK2FhonUEhb
Colorectal Quiz Episode 2 When to redo a PSARP https://staycurrentapp.app.link/RX2eeDqUEhb
Colorectal Quiz Episode 3 Hirschprung Disease https://staycurrentapp.app.link/UnFRkprUEhb
Colorectal Quiz Episode 3.5 Proximal Hirschsprung Disease https://staycurrentapp.app.link/JiaWCGsUEhb
Colorectal Quiz Episode 4 Classic Hirschsprung disease - Surgical Technique https://staycurrentapp.app.link/qGWLoGtUEhb
Colorectal Quiz Episode 5 Proximal Hirschsprung Disease Surgical Technique https://staycurrentapp.app.link/AiGHjcvUEhb
Colorectal Quiz Episode 6 Bowel Management Part 1 https://staycurrentapp.app.link/SVuVYWvUEhb
Colorectal Quiz Episode 7 Bowel Management Part 2 https://staycurrentapp.app.link/b8IhkKwUEhb
Colorectal Quiz Episode 8 Motility Disorders Part 1 https://staycurrentapp.app.link/NRerIoxUEhb
Colorectal Quiz Episode 9 Motility Disorders Part 2 https://staycurrentapp.app.link/s2cVlbyUEhb
Colorectal Quiz Episode 10 Total Colonic Hirschsprung Disease Part 1 https://staycurrentapp.app.link/fEtTMRyUEhb
Colorectal Quiz Episode 11 Total Colonic Hirschsprung's Part 2 https://staycurrentapp.app.link/MNqS9yzUEhb
Colorectal Quiz episode 12 Newborn ARM Part 1 https://staycurrentapp.app.link/x5UL6DBUEhb
Colorectal Quiz Episode 13 Newborn ARM Part 2 https://staycurrentapp.app.link/YqVpTmCUEhb
Colorectal Quiz Episode 14 ARM Newborn Part 3 https://staycurrentapp.app.link/x9mUY7CUEhb
Colorectal Quiz Episode 15 Bowel Management in Spinal Pts. Need for a urologist Part 1 https://staycurrentapp.app.link/etX3mPDUEhb
Colorectal Quiz Episode 16 Bowel Management in Spinal Pts. Need for a urologist Part 2 https://staycurrentapp.app.link/5C7GsJIDEhb
Colorectal Quiz Episode 17 Cloaca Part I https://staycurrentapp.app.link/YGPmYZPEPhb
Colorectal Quiz Episode 18 Cloaca Part II https://staycurrentapp.app.link/vUEzQxG80hb
Colorectal Quiz Episode 19 Hirschsprung Disease - The Obstructed Patient Part 1 https://staycurrentapp.app.link/gBzrAtLKLib
Colorectal Quiz: Episode 20 Hirschsprung Disease – The Obstructed Patient Part 2 https://staycurrentapp.app.link/W7kEcqB6vjb
Colorectal Quiz Episode 21 The History of Hirschsprung Disease https://staycurrentapp.app.link/QXtFg2UlTjb
Colorectal Quiz Episode 22 Hirschsprung Disease - the Soiling Patient Part 1 https://staycurrentapp.app.link/OII38hVhQkb
Colorectal Quiz Episode 23 Hirschsprung Disease The Soiling Patient Part 2 https://staycurrentapp.app.link/DA4WEDIcXlb
Colorectal Quiz Episode 24 Cloaca Part 3 https://staycurrentapp.app.link/3uuEG49mkmb
Colorectal Quiz Episode 25 Perineal Groove https://staycurrentapp.app.link/PxlGWtfswmb
Colorectal Quiz Episode 26 Perianal Crohn's Disease https://staycurrentapp.app.link/qQbadIDjTmb
Colorectal Quiz Episode 27: Delayed Hirschsprung Disease
https://staycurrentapp.app.link/v37xYPDSDnb
Colorectal Quiz Episode 28: Female ARM Management - Perineal Fistula https://staycurrentapp.app.link/lLH7KQr20nb
Colorectal Quiz Episode 30: Tethered Cord https://staycurrentapp.app.link/sE57H6IPzob
Colorectal Quiz Episode 31: Müllerian Anomalies in patients with ARM
https://staycurrentapp.app.link/FuQyrjuC8ob

