Colorectal Quiz: June 26, 2023
Ron Reeder • June 26, 2023
Quiz for June 19th:
Male with ARM newborn colostomy performed. Here is the distal colostogram.
Type of malformation and surgical approach – PSARP only or laparoscopic?
Answer for June 19th Quiz
This distal colostogram shows the defect to be a prostatic fistula (above the elbow), and the distal rectum is above the pubococcygeal (PC) line. So, the best approach is laparoscopic

Quiz for June 26, 2023
For the different types of female ARMs pictured below, what is the name of the malformation and what surgery would you perform?
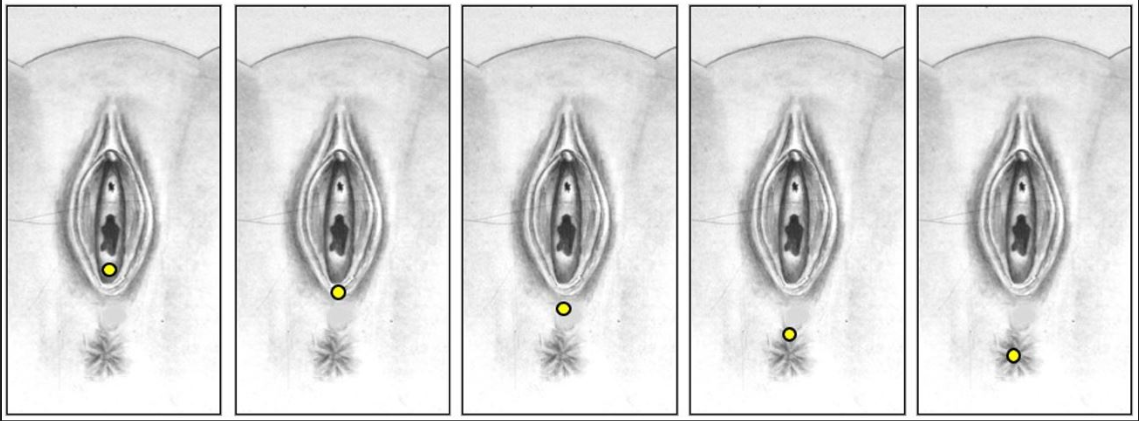
How would you handle this case?

Colorectal Conundrum for January 29: A male with a rectoperineal fistula undergoes a PSARP with mobilization of the rectum, both anterior and posterior rectal walls. In the days following surgery he starts to drain urine around the anoplasty consistent with a urethral injury. He is also voiding via the penis. A cystogram is shown below. How would you manage this situation? Answer: This patient has suffered from a urethral injury, and urine is draining out the posterior urethra into the perineum around the anoplasty. The key first step is to divert the urine with a suprapubic tube. A colostomy is not necessarily needed. The fistula might heal with diversion. If after a month or so a cystogram shows the persistence of the fistula, then a redo is needed with re-mobilization of the rectum, fully lifting the anterior rectal wall off of the urinary tract, and repair the urethra, with coverage of the posterior urethra with an ischiorectal fat pad. Then a voiding trial a month later with ultimate removal of the SP tube.

Colorectal Conundrum for January 22nd: In the previous week’s case, of an imperforate hymen, the MRI showed dilation all the way down to the perineum. Management involved a perineal – introital – incision to drain the fluid. If that were not the case and you had a dilated vagina but the distal extent was far away from the introital area, how might you handle that hydrocolpos? Answer: If this were a case of hydrolpos with normal anus and normal urethra, and the vagina cannot be drained by the introitus like an imperforate hymen, then drainage needs to be from above. IR or laparoscopy is an ideal approach to get a drain in the dilated structure (remember this could be bilateral, so both sides may need to be drained. Drainage is to relieve distension and most concerning its potential cause of distal ureteral obstruction causing hydronephrosis. Once the material hormones have dissipated the hydrocolpos will resolve and can be dealt with later in life via a laparoscopic distal vaginal pull-through, after the onset of puberty. In such a patient, I would follow closely with ultrasound 6 months after thelarche (breast budding).
Colorectal Conundrum for January 16: A newborn female is noted to have abdominal distension. On exam the uretha and anus are normal, and there appears to be a bulge in the hymen. The has an MRI with the image shown below. What would be your treatment plan? What are the variations in such a case and how would you manage each? Answer: This could be a case of imperforate hymen, but the MRI is key – how high up is the obstruction? How large is the hydrocolpos? In this case, it appears that a perineal incision might all that is needed as the dilation extends all the way down to the perineum. That is the most common scenario. An incision at the level of the hymen should drain out the fluid and no further intervention should be needed. Of course a careful exam needs to check to be certain you see a urethra – sometimes such a bulge could be a paraurethral cyst. For the next week’s question – what would you do if the perineal approach was inadequate – i.e. could not reach the dilated lumen.