Colorectal Quiz: June 12, 2023
Quiz for June 5:
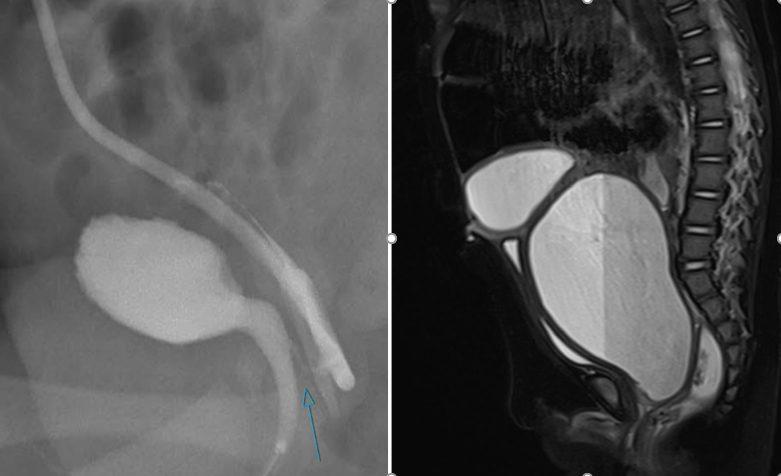
Baby girl, 8 months of age, with a urogenital sinus, and normal anus, without virilization. The imaging is below, contrast study and MRI. The blue arrow shows the vaginal to common channel fistula. Cystoscopy showed a common channel of 2 cm and a urethra length from fistula to bladder neck of 1 cm.
I asked how would you proceed?
Answer for June 5th Quiz
This patient with a UG sinus has a relatively low confluence but with a short urethra – a rare combination. If you did a total urogenital mobilization you would leave the patient with a too short urethra and they would leak urine. Then the option is to do a UG separation. Approaching this from above (laparoscopically or robotically) would be difficult to get to the vaginal-common channel fistula. Approaching that area perineally will also be difficult as there would be inadequate exposure. I would suggest a posterior sagittal approach with an ASTRA (cutting of the anterior rectal wall) or a full transanorectal approach (splitting the rectal wall in the anterior and posterior midline) to gain access. Then with that visualization you could mobilize up the anterior vaginal wall and close the common channel so the urethra becomes a combination of the common channel (2 cm) and the native urethra (1 cm). Then the vagina is pulled through and the rectum closed. It is safe to divert such a case.
Quiz for June 12:
Here is the cloacagram from an 8 month old baby girl. She had a tethered cord which was detethered. What would be your approach? Posterior sagittal only? Total urogenital mobilization? Urogenital separation? How long would you leave the foley in? Would you use a suprapubic tube?

How would you handle this case?

