Colorectal Quiz: February 6, 2023
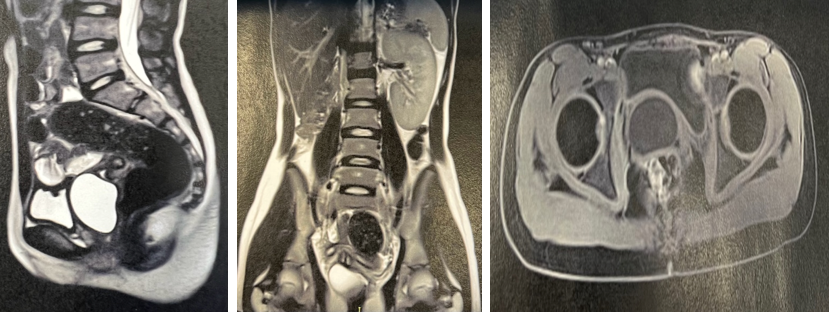
Last week I asked you about A 12-year-old born with an anorectal malformation with a rectoperineal fistula who was treated with dilations alone and has bowel control and only minimal constipation presents with cyclical abdominal pain. She has not yet started to menstruate but has reached thelarche. What do you see on these images? What would be your treatment plan?
The imaging shows a missing right kidney and a pelvic mass on the right – this is an OHVIRA – obstructed hemivagina with ipsilateral renal agenesis. She has not yet started to menstruate, but the accumulated mucous in the blind right hemivagina is causing her pain. On exam, one can feel transvaginally a bulging mass, and this is also visible on the posterior wall of the bladder on cystoscopy. Incision of the septum and excising of it led to drainage of mucous and now an anatomic set-up for future menstrual flow.
For this week, a case sent to us from Clare Skerritt, our colorectal colleague from the UK (on the 3rd anniversary of Brexit).
This is a newborn male with ARM. At 20 hours of life she obtained this cross-fire film.
What would you do? Primary repair or colostomy?

How would you handle this case?
New Paragraph

