Colorectal Quiz: February 13, 2023
Last week I asked you about a case sent to us from Clare Skerritt, our colorectal colleague from the UK (on the 3rd anniversary of Brexit) of a newborn male with ARM. At 20 hours of life, she obtained this cross-fire film. I asked what you would do - a Primary repair or a colostomy?
We have discussed this situation before. The image clearly shows a rectum very close to the perineal skin, so this is amenable to a primary repair. However, you must be aware that this could represent a very low rectobulbar fistula. The principles of repair of opening the posterior rectal wall, and inspected the anterior rectal wall, and mobilizing it up and off of the urinary tract still apply. If you feel confident in your technique this could be done primarily. Of course, the safest route is a colostomy and then a repair followed by colostomy closure, but the morbidity of the stoma and the stoma closure must be weighed into your decision making.

For this week, a 2-year-old boy with ARM and a rectobladderneck fistula after colostomy closure developed a rectogluteal fistula. For this, he was diverted with a new colostomy. On exam, he has a rectal stricture, and the fistula to the gluteal region had healed. This is the pelvic MRI done in anticipation of a redo procedure. What do you see in this image? What would your plan be?
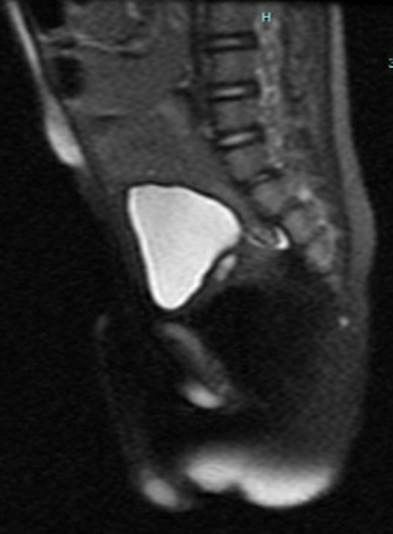
How would you handle this case?
New Paragraph

