COLORECTAL QUIZ: December 20, 2021
For the last two weeks we have been discussing a 12 year old female with lifelong constipation managed with a stool softener who presented with massive abdominal distension, peritoneal findings, and the below xray. She was taken urgently to the operating room and was found to have a sigmoid volvulus.
The surgeons who cared for her untwisted the volvulus, the sigmoid was viable, and decided to perform a sigmoid resection with primary anastomosis. On POD #5 the patient had a leak from that anastomosis, a tiny hole at the staple line, and she underwent re-exploration, and they performed a colostomy with a Hartman’s pouch. I asked you for your plan now.
Below are the contrast studies with colostomy in place, showing the proximal colon and the Hartman’s.
The patient was ruled out for HD by rectal biopsy. An anorectal manometry was normal – but this test was vitally important to inform you whether botox would be needed to treat internal sphincter achalasia. The stoma had been functioning well, so Hartman’s closure can proceed. I would be inclined to check the motility of the proximal segment (CMAN, sitzmark, scintigraphy) to be sure no additional colon should be removed at the time of the colostomy closure. And, based on the constipation history prior to the volvulus would decide whether a Malone should be added to the procedure. Her constipation was not bad, easily managed by medication so a Malone was not felt to be needed here.
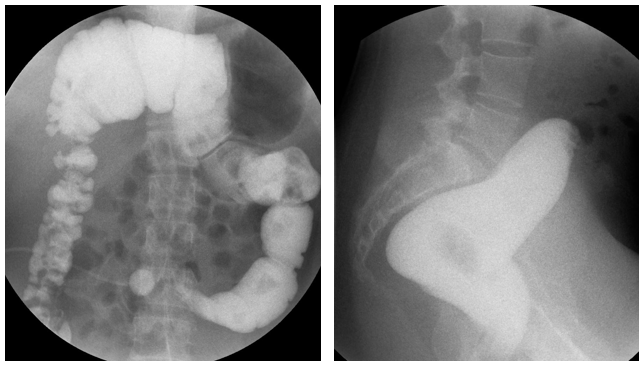
For this week, what would be your plan for this male patient with an ARM and the following distal colostogram. Was this a well-placed initial colostomy?

What would your plan now be?
There’s a new podcast!
Here is the current list of the Colorectal Quiz podcasts, best viewed via the StayCurrent app:
Colorectal Quiz Episode 1: ARM - Low Bulbar Fistula - https://staycurrentapp.app.link/wK2FhonUEhb
Colorectal Quiz Episode 2: When to redo a PSARP - https://staycurrentapp.app.link/RX2eeDqUEhb
Colorectal Quiz Episode 3: Hirschprung Disease - https://staycurrentapp.app.link/UnFRkprUEhb
The Colorectal Quiz Episode 3.5 - Proximal Hirschsprung Disease - https://staycurrentapp.app.link/JiaWCGsUEhb
The Colorectal Quiz Episode 4: Classic Hirschsprung disease - Surgical Technique - https://staycurrentapp.app.link/qGWLoGtUEhb
The Colorectal Quiz Episode 4: Classic Hirschsprung disease - Surgical Technique - https://staycurrentapp.app.link/qGWLoGtUEhb
The Colorectal Quiz Episode 5: Proximal Hirschsprung Disease Surgical Technique - https://staycurrentapp.app.link/AiGHjcvUEhb
The Colorectal Quiz Episode 6: Bowel Management Part 1 - https://staycurrentapp.app.link/SVuVYWvUEhb
The Colorectal Quiz Episode 7: Bowel Management Part 2 - https://staycurrentapp.app.link/b8IhkKwUEhb
The Colorectal Quiz Episode 8 - Motility Disorders Part 1 - https://staycurrentapp.app.link/NRerIoxUEhb
The Colorectal Quiz Episode 9: Motility Disorders Part 2 - https://staycurrentapp.app.link/s2cVlbyUEhb
The Colorectal Quiz Episode 10: Total Colonic Hirschsprung Disease Part 1 - https://staycurrentapp.app.link/fEtTMRyUEhb
The Colorectal Quiz Episode 11: Total Colonic Hirschsprung's Part 2 - https://staycurrentapp.app.link/MNqS9yzUEhb
Colorectal Quiz episode 12 Newborn ARM Part 1 - https://staycurrentapp.app.link/x5UL6DBUEhb
Colorectal Quiz Episode 13 Newborn ARM Part 2 - https://staycurrentapp.app.link/YqVpTmCUEhb
Colorectal Quiz Episode 14: ARM Newborn Part 3 - https://staycurrentapp.app.link/x9mUY7CUEhb
Colorectal Quiz Episode 15: Bowel Management in Spinal Patients - Need for a urologist - https://staycurrentapp.app.link/etX3mPDUEhb
Colorectal Quiz Episode 16: Bowel Management in Spinal Patients - Need for a urologist - https://staycurrentapp.app.link/5C7GsJIDEhb
Colorectal Quiz Episode 17: Cloaca Part I - https://staycurrentapp.app.link/YGPmYZPEPhb
Colorectal Quiz Episode 18: Cloaca Part II - https://staycurrentapp.app.link/vUEzQxG80hb
Colorectal Quiz Episode 19: Hirschsprung Disease - The Obstructed Patient Part 1 - https://staycurrentapp.app.link/gBzrAtLKLib
Colorectal Quiz: Episode 20:- Hirschsprung Disease – The Obstructed Patient Part 2 - https://staycurrentapp.app.link/W7kEcqB6vjb
Colorectal Quiz Episode 21: The History of Hirschsprung Disease - https://staycurrentapp.app.link/QXtFg2UlTjb
The Colorectal Quiz Episode 22: Hirschsprung Disease - the Soiling Patient Part 1 - https://staycurrentapp.app.link/OII38hVhQkb
The Colorectal Quiz Episode 23: Hirschsprung Disease The Soiling Patient Part 2 - https://staycurrentapp.app.link/DA4WEDIcXlb

