Colorectal Quiz: December 5, 2022
Last week I asked how you about the case below, sent to us by our friend Dr. Mansur Nasirov from National Children's Medical CenterTashkent, Uzbekistan. This is a one-year-old male patient with anal stenosis presented and had these radiologic images.
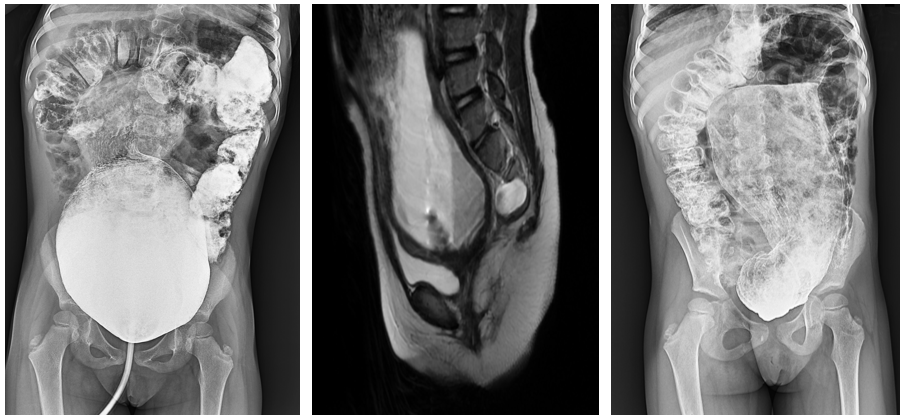
There are several very important considerations here. First – how to treat the anal stenosis. Dilations alone sometimes work, but depending on how long is the narrowed length, a plasty may be required. See these videos for the anal stenosis and rectal atresia scenarios:
Anal stenosis: https://www.expertsinsurgery.com/programs/rectal-stenosismp4-d51c4a?categoryId=49506
Rectal atresia: https://www.expertsinsurgery.com/programs/rectal-atresia-nch-apple-devices-hd-most-compatiblemp4-ee0548?categoryId=49506
Also, the presacral mass must be excised. But is that a teratoma? Or is that a meningocele? You need a spinal MRI to figure out if the mass is connected to the dura. If so, the neurosurgical part should be done independently.
Does this patient need diversion first – yes I think so, and would advocate for either an ileostomy or a proximal sigmoid colostomy.
What to do about the massive rectum and sigmoid? Will that decrease in size over time? I tend to doubt it and might do a pull-through of the normal caliber sigmoid at the time of the anal repair, which is why I like the ileostomy idea. And the mass could also be removed at that time if there is no dural component.
So for me, I would do an ileostomy and then in a few months an anal repair plus pull-through of the healthy sigmoid and removal of the rectum and distal sigmoid, and thereafter ileostomy closure.
I am curious if others have additional thoughts.
For this week, consider this finding in a three-month-old. There is a pit that goes in about 4 cm and parallels the posteriorly rectal lumen. What is it? What would you do about it?

How would you handle this case?
Please note, our weekly quiz is also posted on the Pediatric Colorectal and Pelvic Learning Consortium, (PCPLC) website, www.pcplc.org
https://www.pcplc.org/educational_courses/quizzes
Access code is: pcplc-2022!
Mark your calendars for:
October 26-29, 2023, the 14th Annual Pediatric Colorectal Congress in Milan, Italy.
And
November 16-18, 2023 the Pediatric Colorectal Pelvic Learning Consortium in Scottsdale, Arizona - scientific and didactic programming, for trainees, pediatric surgeons, urologists, gynecologist, gastroenterologists, nurses, APPs, stoma therapists, etc.
Pediatric Colorectal Surgery Tips and Tricks is now out. You can order it using this link: https://bit.ly/Levitt-CRCBooks and this discount code: MAL22.
All proceeds from the sale of the book benefit Colorectal Team Overseas, www.ctoverseas.org
All of our operative videos can be found at www.expertsinsurgery.com and also on the StayCurrent app, the colorectal channel.
Here is the current list of the Colorectal Quiz podcasts, best viewed via the StayCurrent app.
The newest Colorectal Quiz Episode # 34 "Newborn Perforation in ARM" is at the bottom of the list.
Colorectal Quiz Episode 1 ARM - Low Bulbar Fistula
https://staycurrentapp.app.link/wK2FhonUEhb
Colorectal Quiz Episode 2 When to redo a PSARP
https://staycurrentapp.app.link/RX2eeDqUEhb
Colorectal Quiz Episode 3 Hirschsprung Disease
https://staycurrentapp.app.link/UnFRkprUEhb
Colorectal Quiz Episode 3.5 Proximal Hirschsprung Disease
https://staycurrentapp.app.link/JiaWCGsUEhb
Colorectal Quiz Episode 4 Classic Hirschsprung disease - Surgical Technique
https://staycurrentapp.app.link/qGWLoGtUEhb
Colorectal Quiz Episode 5 Proximal Hirschsprung Disease Surgical Technique
https://staycurrentapp.app.link/AiGHjcvUEhb
Colorectal Quiz Episode 6 Bowel Management Part 1
https://staycurrentapp.app.link/SVuVYWvUEhb
Colorectal Quiz Episode 7 Bowel Management Part 2
https://staycurrentapp.app.link/b8IhkKwUEhb
Colorectal Quiz Episode 8 Motility Disorders Part 1
https://staycurrentapp.app.link/NRerIoxUEhb
Colorectal Quiz Episode 9 Motility Disorders Part 2
https://staycurrentapp.app.link/s2cVlbyUEhb
Colorectal Quiz Episode 10 Total Colonic Hirschsprung Disease Part 1
https://staycurrentapp.app.link/fEtTMRyUEhb
Colorectal Quiz Episode 11 Total Colonic Hirschsprung's Part 2
https://staycurrentapp.app.link/MNqS9yzUEhb
Colorectal Quiz episode 12 Newborn ARM Part 1
https://staycurrentapp.app.link/x5UL6DBUEhb
Colorectal Quiz Episode 13 Newborn ARM Part 2
https://staycurrentapp.app.link/YqVpTmCUEhb
Colorectal Quiz Episode 14 ARM Newborn Part 3
https://staycurrentapp.app.link/x9mUY7CUEhb
Colorectal Quiz Episode 15 Bowel Management in Spinal Pts. Need for a urologist Part 1
https://staycurrentapp.app.link/etX3mPDUEhb
Colorectal Quiz Episode 16 Bowel Management in Spinal Pts. Need for a urologist Part 2
https://staycurrentapp.app.link/5C7GsJIDEhb
Colorectal Quiz Episode 17 Cloaca Part I
https://staycurrentapp.app.link/YGPmYZPEPhb
Colorectal Quiz Episode 18 Cloaca Part II
https://staycurrentapp.app.link/vUEzQxG80hb
Colorectal Quiz Episode 19 Hirschsprung Disease - The Obstructed Patient Part 1
https://staycurrentapp.app.link/gBzrAtLKLib
Colorectal Quiz: Episode 20 Hirschsprung Disease – The Obstructed Patient Part 2
https://staycurrentapp.app.link/W7kEcqB6vjb
Colorectal Quiz Episode 21 The History of Hirschsprung Disease
https://staycurrentapp.app.link/QXtFg2UlTjb
Colorectal Quiz Episode 22 Hirschsprung Disease - the Soiling Patient Part 1
https://staycurrentapp.app.link/OII38hVhQkb
Colorectal Quiz Episode 23 Hirschsprung Disease - the Soiling Patient Part 2
https://staycurrentapp.app.link/DA4WEDIcXlb
Colorectal Quiz Episode 24 Cloaca Part III
https://staycurrentapp.app.link/3uuEG49mkmb
Colorectal Quiz Episode 25 Perineal Groove
https://staycurrentapp.app.link/PxlGWtfswmb
Colorectal Quiz Episode 26 Perianal Crohn's Disease
https://staycurrentapp.app.link/qQbadIDjTmb
Colorectal Quiz Episode 27 Delayed Hirschsprung Disease
https://staycurrentapp.app.link/v37xYPDSDnb
Colorectal Quiz Episode 28 Female ARM Management - Perineal Fistula
https://staycurrentapp.app.link/lLH7KQr20nb
Colorectal Quiz Episode 30 Tethered Cord
https://staycurrentapp.app.link/sE57H6IPzob
Colorectal Quiz Episode 31 Müllerian Anomalies in patients with ARM
https://staycurrentapp.app.link/FuQyrjuC8ob
Colorectal Quiz Episode 32 Anorectal Malformations and Cardiac Anomalies
https://staycurrentapp.app.link/3yJWt3t1rqb
Colorectal Quiz Episode 33 Cloacal exstrophy
https://staycurrentapp.app.link/H4l85Pe2isb
Colorectal Quiz Episode 34 Newborn Perforation in ARM
https://staycurrentapp.app.link/EgIRTe14wtb

