COLORECTAL QUIZ: October 17, 2022
Happy Monday!
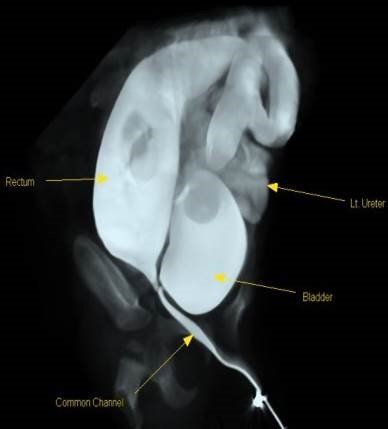
Last week I asked you about a patient with a cloaca, whose anatomy is shown below. I pointed out some highlights: massively dilated left ureter (but MAG III scan showed no distal ureteral obstruction), rectum entering the common channel high, above the PC line, and no evidence of any vaginal connection to the common channel.
Many aspects to this case – the rectum is attached to the common channel and can be mobilized laparoscopically. The common channel will become the urethra. There is no visible vagina, and during the laparoscopy the Mullerian structures need to be inspected. In this case there were none, just normal ovaries and tiny Fallopian tubes on either side. So in the future she will need a vagina, perhaps created with buccal graft or maybe tissue engineered will be available then! I have stopped doing vaginal replacement with colon, unless I need that to bridge the gap to the perineum after a UG separation, but then would have the plan to excise the neovagina in the future and to pull-through the native vagina. If in this case we had found a blind ending but present vagina with a lumen, I would have waited until puberty and then done a laparoscopic mobilization of the distal vagina.
So for this week, we had a patient with HD who initially underwent colonic mapping and an ileostomy. The transition zone was found to be at the splenic flexure. The pull-thru of the splenic flexure went very well, it was pulled down the left side of the abdomen, and we performed a simultaneous closure of the ileostomy. In the postop period the patient had a prolonged ileus, but interestingly passed stool and gas but remained with high volume NG output which was bilious, for 7 days. The abdomen remained flat and the patient was clinically well otherwise. What do you think may be going on, and what would you do about it?
Please note, our weekly quiz is also posted on the Pediatric Colorectal and Pelvic Learning Consortium, (PCPLC) website, www.pcplc.org
https://www.pcplc.org/educational_courses/quizzes
Access code is: pcplc-2022!
How would you handle this case?
Looking forward to seeing many of you soon at the upcoming PCPLC meeting in Cincinnati, November 2-4, 2022: Information for registration found at
www.pcplc.org

Pediatric Colorectal Surgery Tips and Tricks is now out. You can order it using this link: https://bit.ly/Levitt-CRCBooks and this discount code: MAL22.
All proceeds from the sale of the book benefit Colorectal Team Overseas, www.ctoverseas.org
Here is the current list of the Colorectal Quiz podcasts, best viewed via the StayCurrent app.
The newest Colorectal Quiz Episode # 34 "Newborn Perforation in ARM" is at the bottom of the list.
Colorectal Quiz Episode 1 ARM - Low Bulbar Fistula
https://staycurrentapp.app.link/wK2FhonUEhb
Colorectal Quiz Episode 2 When to redo a PSARP
https://staycurrentapp.app.link/RX2eeDqUEhb
Colorectal Quiz Episode 3 Hirschsprung Disease
https://staycurrentapp.app.link/UnFRkprUEhb
Colorectal Quiz Episode 3.5 Proximal Hirschsprung Disease
https://staycurrentapp.app.link/JiaWCGsUEhb
Colorectal Quiz Episode 4 Classic Hirschsprung disease - Surgical Technique
https://staycurrentapp.app.link/qGWLoGtUEhb
Colorectal Quiz Episode 5 Proximal Hirschsprung Disease Surgical Technique
https://staycurrentapp.app.link/AiGHjcvUEhb
Colorectal Quiz Episode 6 Bowel Management Part 1
https://staycurrentapp.app.link/SVuVYWvUEhb
Colorectal Quiz Episode 7 Bowel Management Part 2
https://staycurrentapp.app.link/b8IhkKwUEhb
Colorectal Quiz Episode 8 Motility Disorders Part 1
https://staycurrentapp.app.link/NRerIoxUEhb
Colorectal Quiz Episode 9 Motility Disorders Part 2
https://staycurrentapp.app.link/s2cVlbyUEhb
Colorectal Quiz Episode 10 Total Colonic Hirschsprung Disease Part 1
https://staycurrentapp.app.link/fEtTMRyUEhb
Colorectal Quiz Episode 11 Total Colonic Hirschsprung's Part 2
https://staycurrentapp.app.link/MNqS9yzUEhb
Colorectal Quiz episode 12 Newborn ARM Part 1
https://staycurrentapp.app.link/x5UL6DBUEhb
Colorectal Quiz Episode 13 Newborn ARM Part 2
https://staycurrentapp.app.link/YqVpTmCUEhb
Colorectal Quiz Episode 14 ARM Newborn Part 3
https://staycurrentapp.app.link/x9mUY7CUEhb
Colorectal Quiz Episode 15 Bowel Management in Spinal Pts. Need for a urologist Part 1
https://staycurrentapp.app.link/etX3mPDUEhb
Colorectal Quiz Episode 16 Bowel Management in Spinal Pts. Need for a urologist Part 2
https://staycurrentapp.app.link/5C7GsJIDEhb
Colorectal Quiz Episode 17 Cloaca Part I
https://staycurrentapp.app.link/YGPmYZPEPhb
Colorectal Quiz Episode 18 Cloaca Part II
https://staycurrentapp.app.link/vUEzQxG80hb
Colorectal Quiz Episode 19 Hirschsprung Disease - The Obstructed Patient Part 1
https://staycurrentapp.app.link/gBzrAtLKLib
Colorectal Quiz: Episode 20 Hirschsprung Disease – The Obstructed Patient Part 2
https://staycurrentapp.app.link/W7kEcqB6vjb
Colorectal Quiz Episode 21 The History of Hirschsprung Disease
https://staycurrentapp.app.link/QXtFg2UlTjb
Colorectal Quiz Episode 22 Hirschsprung Disease - the Soiling Patient Part 1
https://staycurrentapp.app.link/OII38hVhQkb
Colorectal Quiz Episode 23 Hirschsprung Disease - the Soiling Patient Part 2
https://staycurrentapp.app.link/DA4WEDIcXlb
Colorectal Quiz Episode 24 Cloaca Part III
https://staycurrentapp.app.link/3uuEG49mkmb
Colorectal Quiz Episode 25 Perineal Groove
https://staycurrentapp.app.link/PxlGWtfswmb
Colorectal Quiz Episode 26 Perianal Crohn's Disease
https://staycurrentapp.app.link/qQbadIDjTmb
Colorectal Quiz Episode 27 Delayed Hirschsprung Disease
https://staycurrentapp.app.link/v37xYPDSDnb
Colorectal Quiz Episode 28 Female ARM Management - Perineal Fistula
https://staycurrentapp.app.link/lLH7KQr20nb
Colorectal Quiz Episode 30 Tethered Cord
https://staycurrentapp.app.link/sE57H6IPzob
Colorectal Quiz Episode 31 Müllerian Anomalies in patients with ARM
https://staycurrentapp.app.link/FuQyrjuC8ob
Colorectal Quiz Episode 32 Anorectal Malformations and Cardiac Anomalies
https://staycurrentapp.app.link/3yJWt3t1rqb
Colorectal Quiz Episode 33 Cloacal exstrophy
https://staycurrentapp.app.link/H4l85Pe2isb
Colorectal Quiz Episode 34 Newborn Perforation in ARM
https://staycurrentapp.app.link/EgIRTe14wtb

