Colorectal Quiz: February 27, 2023
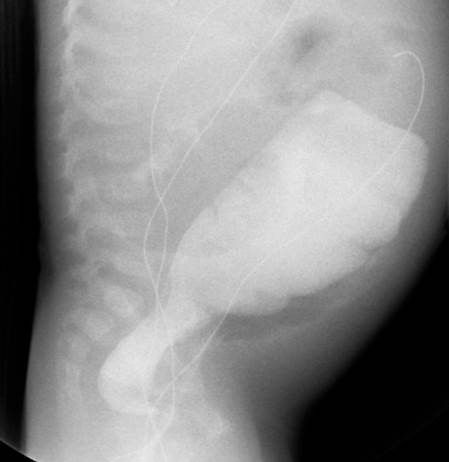
Last week I asked about a 16-month-old male who presented with chronic distension and failure to thrive. Rectal biopsy confirmed suspicion for Hirschsprung disease. How would you proceed?
This old diagnosed HD case looks to have a transition zone in the upper rectum/lower sigmoid. Given the amount of distension and the failure to thrive, a diversion is indicated. I would recommend a laparoscopic biopsy of the sigmoid – it likely will show ganglion cells and a diversion with an ileostomy. If on frozen section the sigmoid shows ganglion cells, no further mapping is needed. In the future, the patient can have their pull-through, with ileostomy closure later or even at the same time.

For this week: An 8-month-old female presents with passage of stool via the vaginal opening – the introitus and the anus are otherwise normal.
How do you confirm your suspicion of an H-type rectovaginal fistula?
Does the patient need a diversion?
How would you repair it?
How would you handle this case?
New Paragraph

